
Dental
ImageWorks Generations of Imaging
For more than 35 years, ImageWorks has been providing the best in imaging solutions to dental health professionals. ImageWorks’ objective is to improve both patient care and practice efficiency by offering solutions that perform at the highest level while seamlessly integrating with your existing technology. ImageWorks understands that technology should conform to the patient, not the other way around.
Imageworks’ Panoura 18S Dental Panorammic X-Ray
PRODUCT CODE: PAN18S

The Panoura 18S is the most practical advanced 2D dental imaging system. Ideal for doctors who need ultra-high-resolution Panoramic and Ceph capabilities all in one compact, low-cost platform.
DIRECT CONVERSION SENSOR
Most Panoramic CMOS sensors use lower cost, more generally available materials that are less sensitive to x-ray. Therefore, these sensors must convert x-ray to light before converting to a digital signal. This can result in image blurriness because the extra conversion step can cause the radiation to “fan out” and inadvertently trigger surrounding pixels. The Panoura has a unique sensor design that converts x-ray directly to digital, which contributes to a much sharper image.
16 BIT SENSOR
How do we create the gorgeous images we’re so well-know for? It’s the 16 bit sensor. A 16 bit sensor has twice as many greyshades that can be presented in each pixel as a 15 bit sensor and four times as many as a 14 bit sensor. In the end, a 16 bit sensor provides fantastic texture and contrast.
FMX CLIPPINGS & BITEWINGS
Not only do we do create bitewings, but our FMX Clipping feature creates 18 intraoral-sized images clipped from the pan with one click. Instead of taking 18 individual images with an intraoral X-Ray, they can all be generated at once in 14 seconds.
EXQUISITE IMAGES – EVEN WITH SUBOPTIMAL POSITIONING
Panoura 18S features auto-correction for suboptimal patient positioning. Without this, an already suboptimal image (from a pan with a lower-quality sensor) can be further degraded if the patient is not positioned optimally. With the Panoura, the very high data-capture sensor acquires many “layers” of image data. This allows the powerful software to auto-correct for suboptimal patient positioning. It’s worth noting that all of this data is available after the image is taken – so the image can be further optimized if desired. In the end, this assures exquisite images with the Panoura every time while being less dependent on operator training or the ability of the patient to remain stationary.

EASY 3D UPGRADE
Our basic 2D panoramic unit is upgradeable to 3D, so there is peace of mind that the initial investment is protected if 3D capability is needed later on.
SMALL FOOTPRINT
The Panoura’s small footprint makes it an incredibly practical solution for tight offices.
Imageworks’ ImageScan HD
PRODUCT CODE: IMAGESCANHD

ImageScan HD
The next generation in our proud legacy of x-ray technology.

DC Intraoral X-Ray – ImageScan HD
Best Image First Time Every Time — Power Factor Correction assures highly stable and consistent output regardless of quality of input power source.
Reduced Dosage — Patented shielding method makes leakage close to zero. The DC system significantly reduces harmful soft radiation, compared to conventional AC type machines.
Long Lasting Quality — Life cycle tested both mechanically and electrically over 200,000 cycles. Assures the unit will last.
Mobile Intraoral X-ray – Mobile ImageScan HD
PRODUCT CODE: MOBILEIMAGESCANHD

One Unit for Multiple Operatories — Make your X-Ray unit work for you by leveraging your investment across many different operatories.
Easy Installation
No wall mounting or invasive construction work to your office.
Small Footprint
Compact design allows it to fit in many tight spaces.
Best in Class Performance
All the same dosage and image quality advantages of ImageScan HD, but now it’s mobile!
Five Crucial Questions to Ask When Buying a Dental Intraoral X-Ray Unit
Whether you are installing a dental intraoral x-ray in a new office, or you need to replace an old unit, it’s helpful to go into the process eyes wide open. In many cases, the questions below can be answered by the company providing your dental intraoral x-ray. However, it helps to understand all the requirements so that there are no surprises that cause delays or additional costs.
1. Does it matter whether it’s a DC or AC x-ray? To answer this, it’s worth a quick explanation of the fundamental difference between a DC x-ray and an AC x-ray. Both types of wall mounted intraoral x-rays in a dental office (whether it is a DC x-ray or an AC x-ray) are powered by basic AC electricity that comes from the wall. The difference between a DC x-ray and an AC x-ray lies in what they do with that incoming electricity.
The incoming AC electricity is like a sine wave: it has pulses that go up and down. The power level (or intensity) of the x-ray generated by an AC x-ray matches this sine wave shape, and the actual x-ray power coming out of the machine oscillates at 60 times per second – like the input electricity.
A DC dental intraoral x-ray changes this input electricity so that the x-ray coming out of the unit is a single pulse that maintains more of a consistent power level through the entire exposure.
This difference in the profile of the x-ray output results in two subtle effects.
First, the “up and down” nature of the AC x-ray output creates more radiation when all other parameters are equal. Every time the power level is below a certain threshold, it is emitting radiation that is not having an impact on image quality (some refer to this as “soft radiation”). In other words, there is a small dose to the patient, but because it is below the sensitivity threshold of the film or sensor that’s capturing the image, it has no impact on the image. For AC x-ray, the power level is dipping below this threshhold 60 times per second, and therefore is emitting more of this soft radiation than a DC intraoral x-ray.
Second, there may be less consistent image quality when all other parameters are equal. If your exposure is 0.04 seconds in duration (not an uncommon setting), that’s only 2.5 “pulses” with an AC x-ray (because they occur 60 times per second). However, depending on the exact timing, the reality of that particular exposure could be 3 “peaks” and 2 “valleys”, or could be the other way around. This difference can create a slight inconsistency in the amount of exposure the sensor or film actually receives. In other words, two exposures taken with exactly the same parameters may have slightly different levels of energy applied to the sensor for an AC x-ray.
You may ask: why would anyone buy an AC x-ray? The answer is two-fold. First, there may be a price advantage with the AC x-ray. Second, the differences in both dosage and radiation are very slight, and both of these results are well within the federal requirements for these pieces of equipment.
2. Do I need a different dental intraoral x-ray if I am using film instead of digital sensors? The short answer is: typically no.
Typically, the amount of x-ray energy required to generate ideal images with film is higher than that required for a digital sensor. However, almost all intraoral x-ray units today have the ability to adjust settings. For most intraoral x-ray units, increasing the output power is done by simply switching the unit to a mode that increases the time (or duration) of the exposures (typically this is shown in milliseconds, or ms).
As an aside, if you are using film, the ideal parameters would also vary depending on which type of film you use (D speed, E speed, F speed, etc). Film speeds labelled as “slower” (like D-speed) require more energy to create the image than “faster” film speeds (like F-speed).
3. What shielding is required in the office? The official requirements will vary by state (and in some cases, by locality). However, here are some guidelines to consider.
The two most common characteristics of the office that are typically specified as requirements for intraoral x-ray operation are distance and wall material (sometimes referred to as “distance and density”). The reason for this is that these are two very effective protections against radiation.
Sometimes simply having 6 feet spacing between the intraoral x-ray and an operator is sufficient and no walls are required. Sometimes, a basic wall (typically referred to as “drywall” or “gypsum”) is required to separate the x-ray and the operator. Typically, most states will have some variation of these requirements. Rarely are lead-lined walls required for intraoral x-rays in dental offices. However, some state may require this if there is a very high volume of exposures being taken.
4. Can I have my repair person install my intraoral x-ray? Most states require that the intraoral x-ray be installed by a person who has registered with the state as a qualified installer. Therefore, if your repair guy has registered, then: “yes”. Otherwise, you want to make sure you are using a certified installer.
One of the ways the FDA monitors this is through a form that is filled out by the installer called the FDA 2579 form. The installer is required to complete this form, and then send one copy to the FDA and one copy to the state. A third copy is provided to the office, which is responsible for keeping a copy of this form to document that the piece of equipment was properly installed. It’s important to keep your copy, because it is common in many states that an inspector will come to the office periodically asking to see this document for each x-ray unit.
5. Do I need a wall-mounted unit, a mobile unit, or a handheld unit? This is a fundamental question that depends on your office needs. Handheld and mobile x-rays offer some economies of scale as they can be shared between rooms. However, there are performance aspects of a wall-mounted and a mobile unit that are often preferable to a handheld x-ray. For more on this question, see our post sharing more detail on these tradeoffs:
The intraoral dental x-ray is a critical component to a busy dental practice. Understanding some of key components involved in having a new intraoral x-ray installed in your office will help your team make sure there are no surprises.
If you have any questions about this process, please give us a call to talk to one of our specialists.
Imageworks’ T-100 Handheld X-Ray
PRODUCT CODE: T-100

Save the cost of multiple wall-mounted x-rays
Portable – go to any treatment room
No walking back and forth in and out of the room between exposures
Stay by your patient’s side.
Allows you to ease your more challenging patients.
Freedom in workflow that can’t be matched by a wall-mounted x-ray
Sharp images that you can count on
0.4 mm focal spot
70 kV output yields strong contrast resolution
Ideal for film or digital
Scattershield provides superior protection from scatter radiation
Internal lock-tight shielding eliminates backward radiation from the X-Ray source

Full FDA Approval. Compliant in every state except for NE, MO, NC, SC
Light weight Neck strap reduces load on the clinician and allows hands-free to adjust patient positioner
Lightweight and high-quality lithium-ion battery
Plug and play
90 minutes for full charge
Lasts all day on single charge (400 exposures)
Intuitive interface

Comfortable and ergonomic
Imageworks’ Dental CBCT and Panoramic X-Rays
Dental CBCT and Panoramic X-Rays
PRODUCT CODE: PANX-ERA-CBCT

The sensor used in a Dental CBCT or panoramic system is like the engine of an automobile: the component that defines the system’s performance. You are investing a lot of your hard-earned money in this piece of equipment. Do you know what’s under the hood?
Features:
0.2 mm focal spot (smallest in the industry)
16 bit sensor (highest in the industry)
Direct Conversion sensor
Manufactured in Japan
Clip FMX from Panoramic
Easy to Use and a Great Price
Integrates with all Major Software
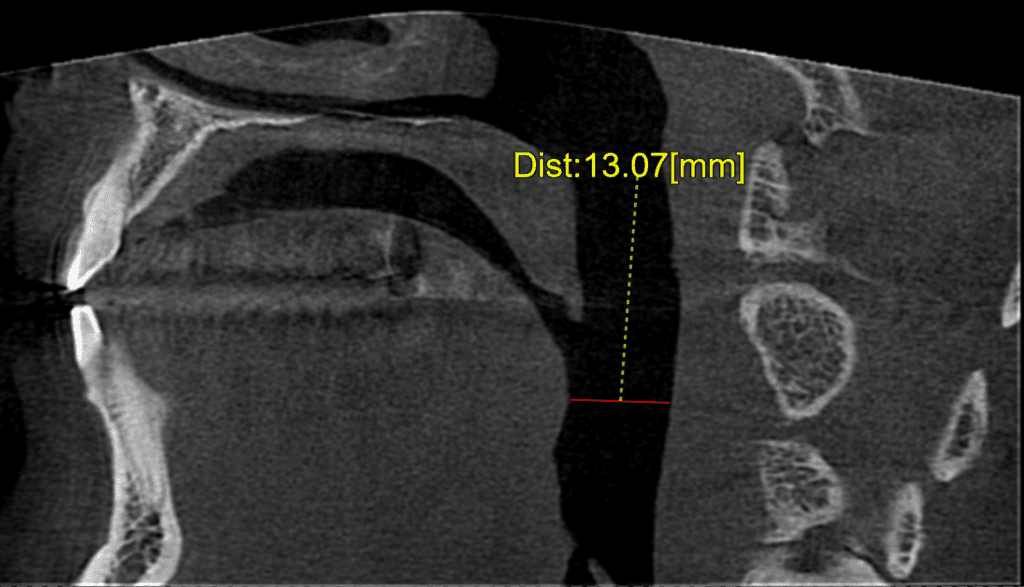
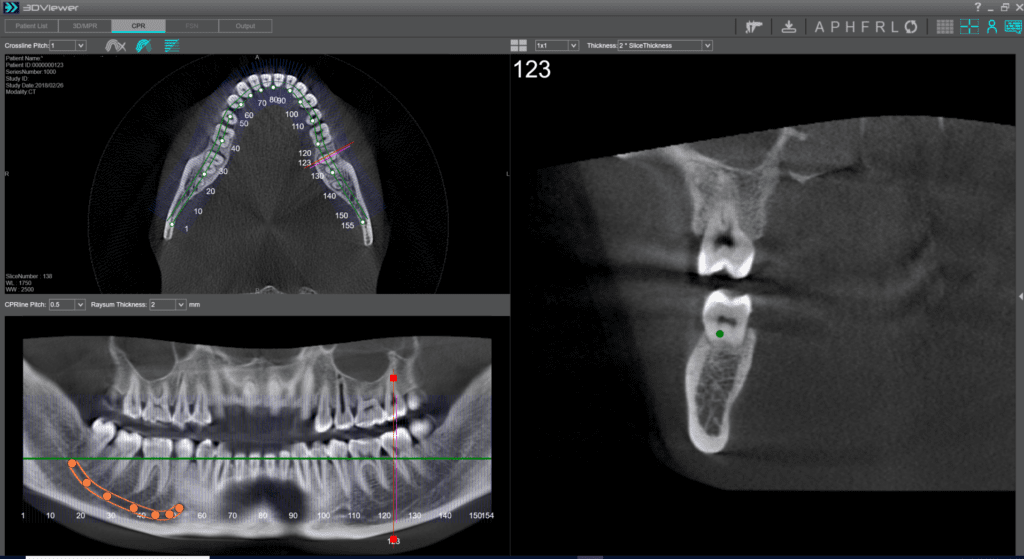
Multiple Fields of View from 6 cm x 4 cm up to 16 cm x 8 cm
Ideal for all applications including Endo, Implants and Airway
Gorgeous Image quality at all levels
Low dosage mode emits less radiation than a traditional intraoral FMX exam
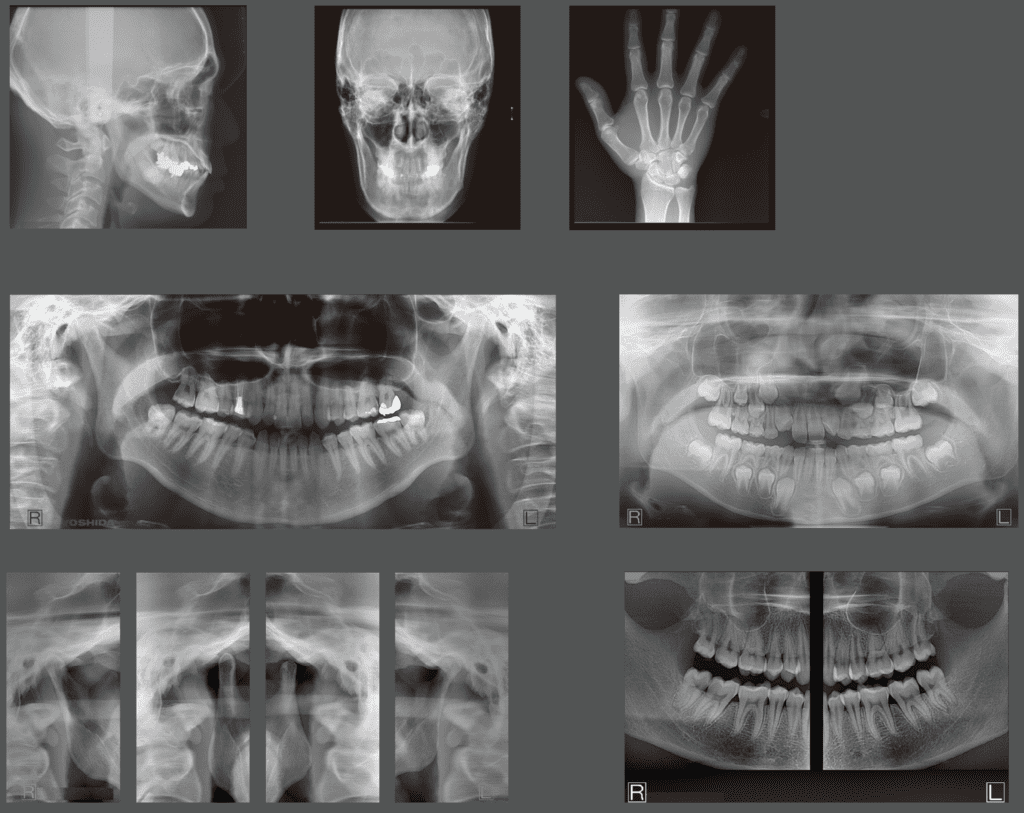
Sample Images:

0.2 Focal Spot 
0.5 Focal Spot 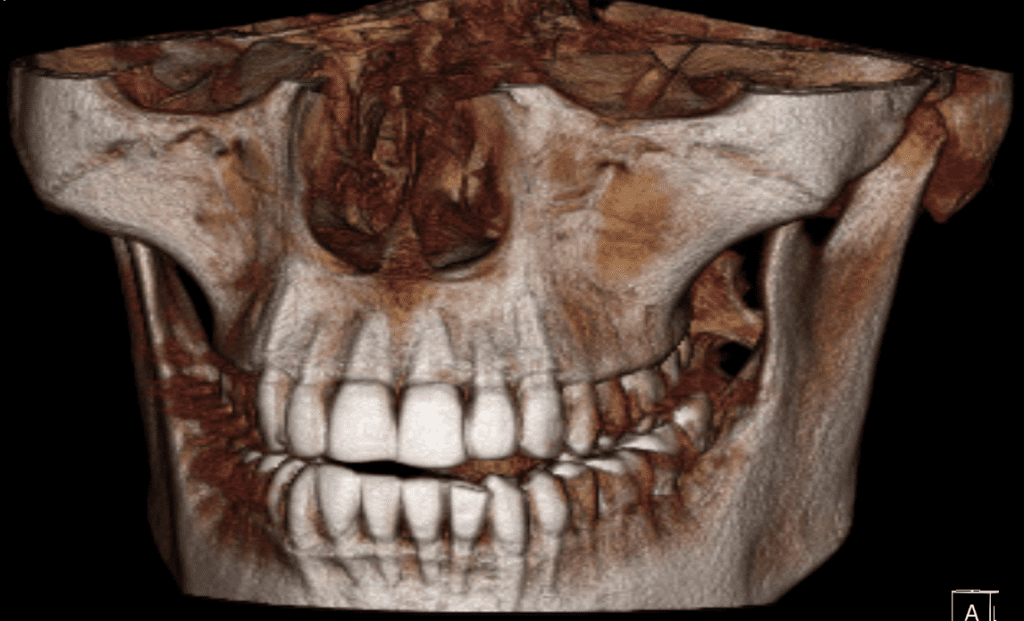
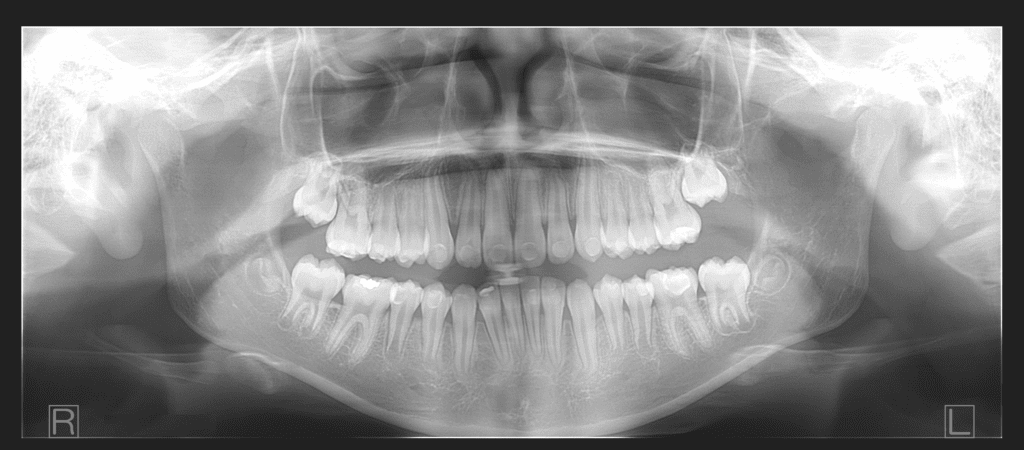


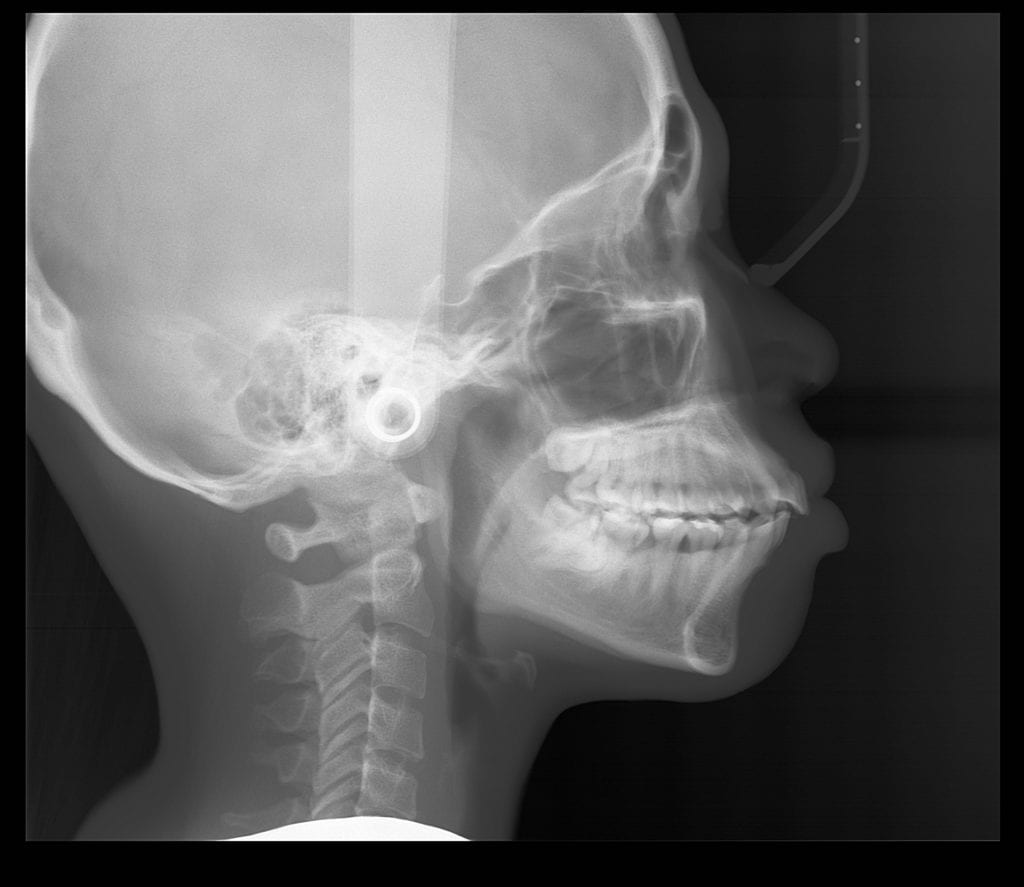
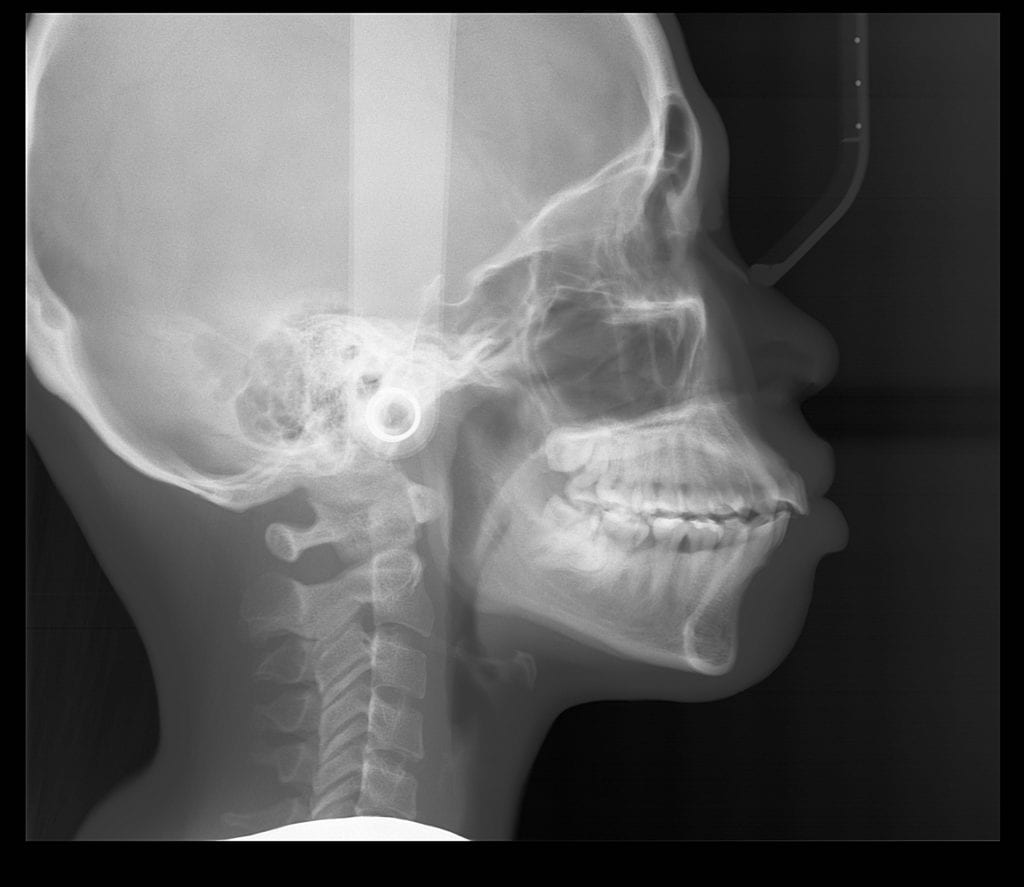
2D Panoramic and Ceph Images in Ultra HD
Direct Conversion Sensor avoids extra transition step that degrades image quality with most panoramic x-ray sensors
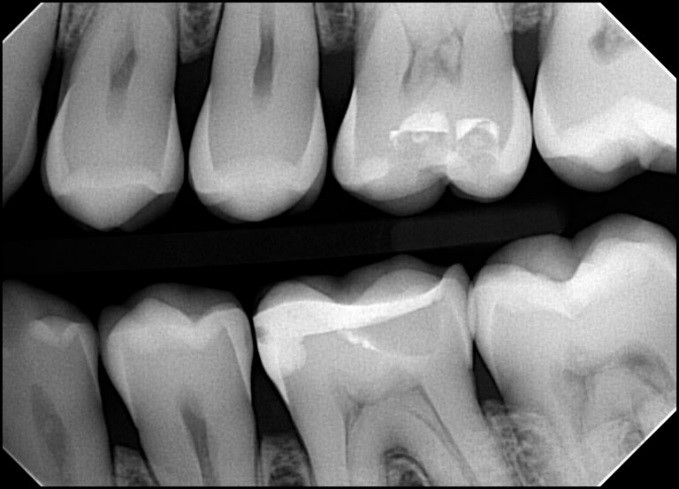
TMJ and bitewings
Captures over 50 different panoramic layers in every scan so that even if technique is less than perfect, a fantastic image can be achieved
16 bit sensor creates best-in-class contrast resolution
2D images integrate with most major imaging software platforms
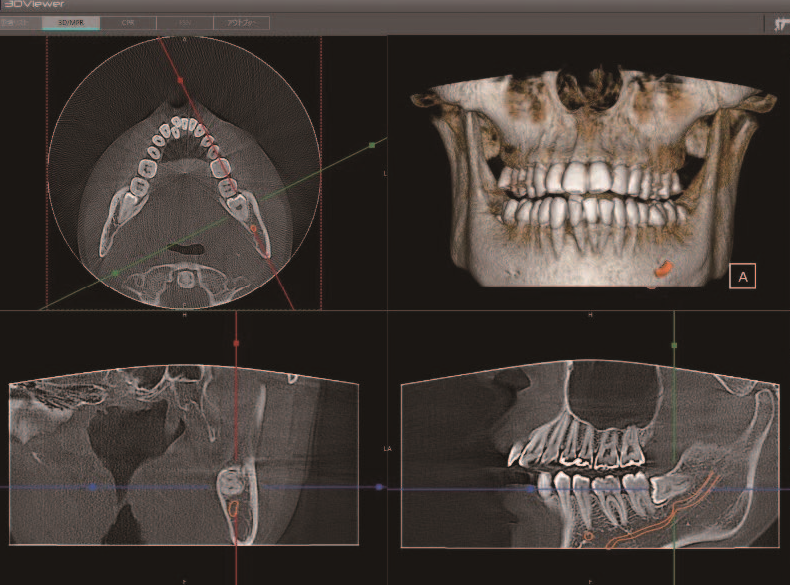
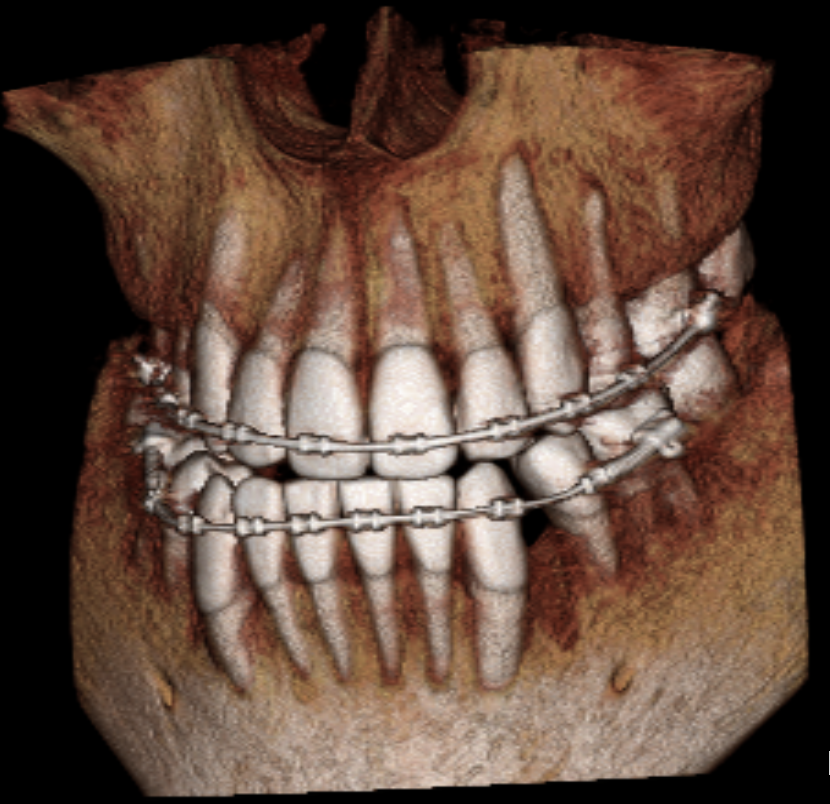
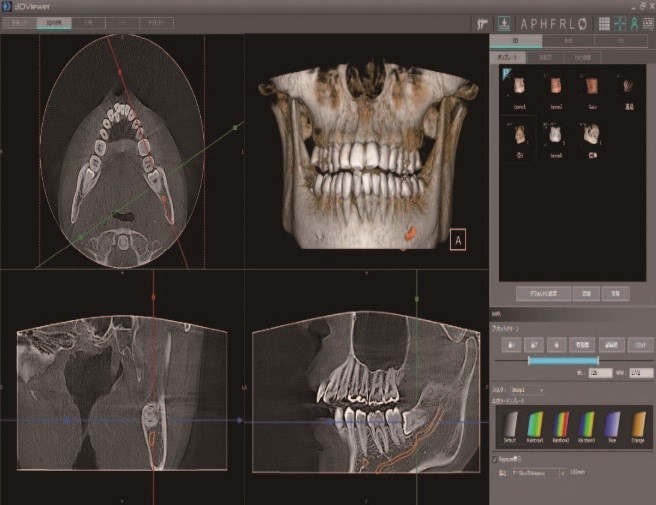
3D images viewed throughout the office
3D volumes are DICOM standard so can easily be imported into most major 3D imaging software, or used with any lab service
3D volume can be converted to STL format
Colleagues can view 3D volumes sent to them even if they have no software other than Windows
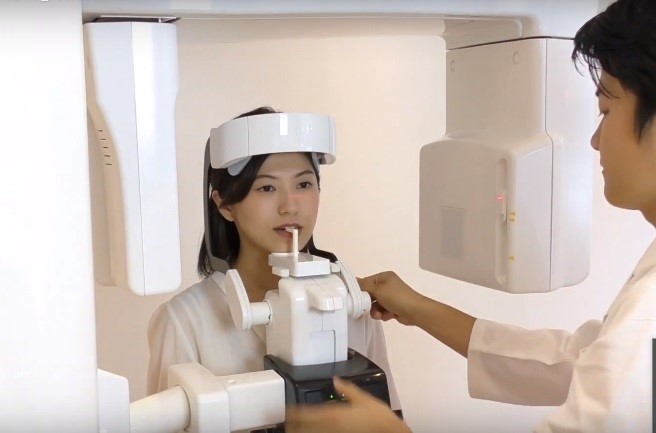
Front-viewing patient positioning
Ceph model has option of dedicated ceph sensor
360 degree rotation
Intuitive interface means less training and no mistakes
Simple positioning also enhances patient comfort
Integrates with all Major Software
EVA SELECT DIGITAL SENSORS
EVA SELECT DIGITAL SENSORS
PRODUCT CODE: EVASELECT1, EVASELECT2
*same product; two different sizes

ImageWorks’ EVA Select digital sensors leverage CMOS technology to provide high resolution, diagnostic-quality images with wide latitude, sharp clarity and enhanced contrast. Whether you are converting to digital for the first time, or expanding your existing capabilities, we can help you.